How it works in practice.
Capture · Document · Connect.
Capture
Ailacra Ambient flow
When the conversation is the note.
- 1 Open — Tap the patient and start capture.
- 2 Talk — The conversation in the room is captured. Hands-free at the bedside.
- 3 Pause / Resume — Step out for the next patient; return without losing the thread.
- 4 Review — AI drafts the narrative; you confirm clinical findings.
- 5 Insert — Copy the finished note into your EMR.
Ailacra Template flow
You choose what to document. Not a form.
- 1 Open Template — Pick the chief complaint or mechanism (MVA, chest pain, GSW, … 120+ more).
- 2 Mark — Circle for present, backslash for absent. Single tap; no typing.
- 3 Expand — Tap a finding to open a subtemplate for finer detail when you want it.
- 4 Generate — AI curates the differential and writes the narrative.
- 5 Code & Insert — ICD-10, CPT, and MDM are assigned; one-click insert into the EMR.
See it in motion — a cholecystitis encounter, charted in real time
Chart as you go. Capture in the room.
Document
Two examples of how Template marks and anatomic drawings become physician-quality narrative.
Mark. Review.
Circle and backslash findings. AI writes the note.
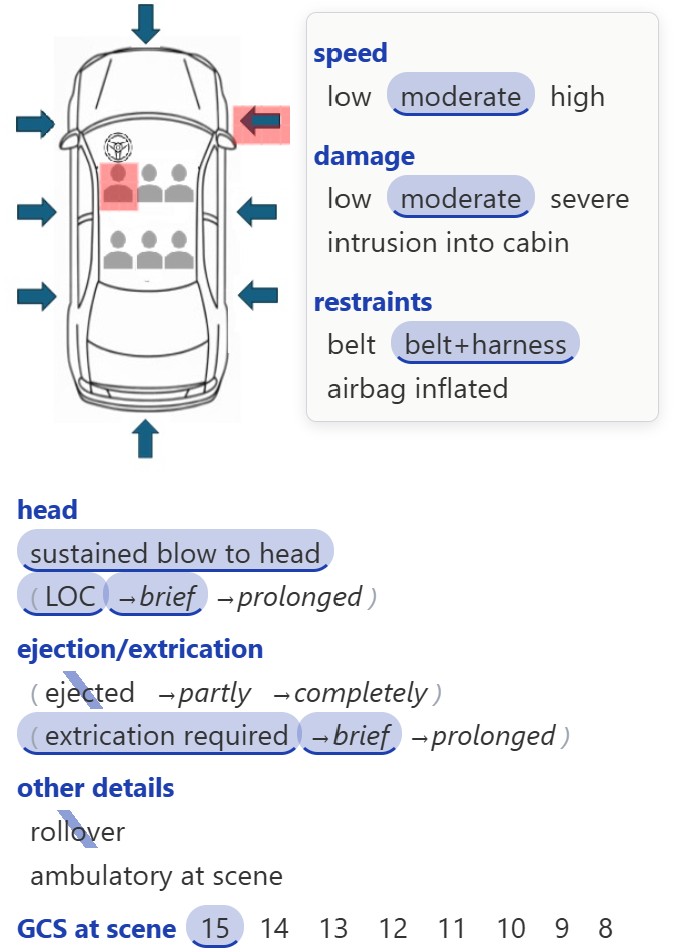
CHIEF COMPLAINT: MVA
Historian: patient (good historian)
HISTORY OF PRESENT ILLNESS: This 55 YO male presents after an MVA that occurred just prior to arrival. He was the driver of the vehicle when it was struck from the front right side at a moderate speed, resulting in moderate vehicle damage. There was no rollover involved. He was utilizing both a seat belt and harness at the time of the impact. He required a brief extrication from the vehicle but was not ejected. He sustained a blow to the head and experienced a brief loss of consciousness, although he maintained a GCS of 15 at the scene.
Draw it. Read it.
A single stroke on the anatomic diagram becomes a complete clinical description.
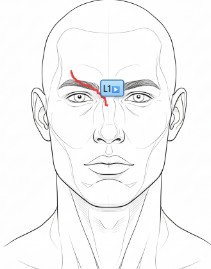
PHYSICAL EXAM:
Head: Laceration beginning at the right paramedian forehead, extending through the central forehead, glabella, nasion, and nasal bridge, and ending at the left paranasal area.
Lacerations, burns, GSW, shrapnel, ecchymosis — draw the finding, get the description.
Connect
Two ways into the EMR — pick whichever your hospital supports.
Inside the EMR — SMART on FHIR
Ailacra Embedded launches straight from the patient chart.
Open Ailacra straight from the patient chart. SMART on FHIR carries the patient and encounter context across automatically.
Paste the finished narrative back into the EMR with a single tap — or copy to clipboard for systems without write-back.
Medications, allergies, problem list, surgical history, and lab results pull in automatically. Repeat values (e.g., serial troponins) are handled cleanly.
No-Interface Mode — Scan. Capture. Paste.
No SMART integration needed. Works with Epic, Oracle Health, Meditech, Athena, and anything else.
Scan the wristband or sticker, capture in Ambient or Template, paste the note into any EMR.